
|
|
Rim Lesions | Concentric Tears | HIZ Sign | Anular Tear Home | Discography
Radial Anular Tears: (aka: radial fissures)
 A
radial anular tear is any annular tear that begins within the center
of the disc (nucleus pulposus) and progresses in an outward or radial. There are five different categories of radial annular tears (grade I - V) which we will discuss further below.
A
radial anular tear is any annular tear that begins within the center
of the disc (nucleus pulposus) and progresses in an outward or radial. There are five different categories of radial annular tears (grade I - V) which we will discuss further below.
Radial tears which will reach the outer one third of the posterolateral annulus are believed to be symptomatic and the main cause of internal disc disruption (IDD, discogenic pain syndrome). They are also believed to be the major cause of patients with isolated disc resorption.
Figure #1 shows a 'full-thickness Radial tear (Grade III) that completely bisects the disc. This particular tear would be classified as a 'Grade 3 radial tear in accordance with the 'modified Dallas Discogram naming system, which is the 'gold standard' when it comes to describing these tears.
Radial anular tears are strongly associated with disc degeneration (3) which makes the annulus fibrosus more dry and brittle, and may be a consequence of a single traumatic event, repetitive trauma, and/or poor genetics for the materials that the annulus fibrosus are constructed of (type II and III collagen).
Nuclear ‘cleft’ formation, which are cracks that occur within a degenerated nucleus, are thought to be the precursors for the formation of a radial tear. With time and/or trauma these nuclear clefts will progress outwardly (radically) in a parallel or obliquely parallel fashion. Although radial annular tear usually occur in the L5 disc (they occur in this disc more frequently than all the other discs put together), there also commonly seen in the L4 disc and less commonly seen in the others. [3]
Occasionally, radial tears will merge into a pre-existing rim-lesion or concentric tear in the periphery. This merger often results in the appearance of an HIZ (High Intensity Zone) on MRI, which is the least invasive way to diagnose an anular tear.
It is important to understand that NOT ALL RADIAL TEARS ARE PAINFUL, and that they are often found in asymptomatic patients (21). Why some tears are extremely painful and some aren’t, is still not completely understood. The current theory states that if nuclear material migrates into the outer region of the annulus, which is well innervated with pain sensitive (nociceptive) nerve fiber, a chemical irritation and inflammation process occurs around these now exposed nociceptors (pain triggers at the beginning of sensory nerve fiber) and causes discogenic pain. Another theory is that the degenerated and damaged nucleus pulposus can no longer support its share of the axial load of the body. Biomechanical studies have indicated that following an annular tear, axial load is no longer carried in the center of the disc but instead shifts posteriorly right over the nerve-infested posterior and posterolateral annulus fibrosus. Therefore, in addition to a painful inflammatory reaction, now you get a mechanical (a grinding) irritation of those already inflamed and irritated nociceptive fibers. Another theory is that an autoimmune reaction occurs when the virgin nucleus pulposus cells get into the posterior annulus.
Empirically speaking, it is well-known that symptomatic annular tear are very difficult to treat and arguably the most effective treatment is the passage of time, and I mean a lot of time! The general rule of thumb is this: if you're not better by four months, you probably won't be a whole lot better at 18 months. But, barring serious reinjury, by 4-5 years, you should be doing pretty good – but not perfect.
 Research has demonstrated that a full thickness (grade III) annular tear will eventually develop a "plug" of granulation tissue which will finally stop the leakage of nucleus pulposus chemicals (cytokines) into/onto the nerve fibers in the posterior disc. that should remove the chemical irritation; however, the biomechanical axial load posterior-shift is unable to be fixed (unless you have fusion).
Research has demonstrated that a full thickness (grade III) annular tear will eventually develop a "plug" of granulation tissue which will finally stop the leakage of nucleus pulposus chemicals (cytokines) into/onto the nerve fibers in the posterior disc. that should remove the chemical irritation; however, the biomechanical axial load posterior-shift is unable to be fixed (unless you have fusion).
Figure #2, show what this tissue plug may look like. Both animal and cadaver studies demonstrate this neovascularization / granulation plug phenomenon. Animal studies have shown that this vascularized granulation tissue appears within a few months after the artificial creation of an annular tear (Rim Lesion) in the outer anulus.
Another drawback to the healing process is the fact that the granulation tissue plug fails to seal the entire annular tear. Research has demonstrated that only the outer one third of the annulus actually heals. [5] Therefore, once you get an annular tear, the disc tissue in that region is never as strong as it used to be and those affected will be prone to flareups of periodic low back pain.
Other research has demonstrated that if scar tissue does happen to close the entire annular tear, then nociceptive nerve fiber grows all the way into the center of the disc because it followed the new blood vessel formation.
The Dallas Discogram Description: A classification system for radial tears.
Not all radial anular tears are alike. Most radial tears only extend partially into the anulus and do not reach the pain sensitive out 1/3 of the anulus. Therefore it became important to develop a way to classify the severity of these radial tears. Enter the Dallas Discogram Description.
The ‘Modified Dallas Discogram Description’ was finalized in the 1990’s and is the Gold Standard for the classification of Radial anular tears. It was initially developed by a group of researcher from Texas (14) and then ‘modified’ by Bogduk et al (7), and finally Schellhas et al (15). In a nutshell, the nucleus of the suspected disc will be injected with a contrast material, that will out-line the nucleus and/or and leaking tears. After a short time, the patient is taken to the CT and axial pictures of the disc are made. If the nucleus is ripped, the dye will have migrated down the tear. The degree of disc disruption is described by how far this dye migrates away from the center of the disc.
 There
are six possible categories that describe the severity of the radial
anular tear. The grade 0 is a normal disc; where no contract material
leaks from the nucleus. The grade 1 tear will leak contrast material
only into the inner 1/3 of the anulus. The grade 2 tear will leak
contrast through the inner 1/3 and into the middle 1/3 of the disc. The
grade 3 tear will leak contrast through the inner and middle anulus.
The contrast spills into the outer 1/3 of the anulus. The grade
4 tear further describes a grade 3 tear. Not only does the contrast
extend into the outer 1/3 of the anulus, but it is seen spreading concentrically
around the disc. To qualify as a grade 4 tear the concentric spread
must be greater than 30 degrees. Pathologically, this represents the
merging of a full thickness radial tear with a concentric anular tear.
The ‘evil’ grade 5 tear describes either a grade 3 or grade
4 radial tear that has completely ruptured that outer layers of the
disc and is leaking contract material out of the disc. This type of
tear, which I most likely suffered from, can cause a chemical radiculopathy
in one or both of the extremities and result in the dreaded sciatica.
There
are six possible categories that describe the severity of the radial
anular tear. The grade 0 is a normal disc; where no contract material
leaks from the nucleus. The grade 1 tear will leak contrast material
only into the inner 1/3 of the anulus. The grade 2 tear will leak
contrast through the inner 1/3 and into the middle 1/3 of the disc. The
grade 3 tear will leak contrast through the inner and middle anulus.
The contrast spills into the outer 1/3 of the anulus. The grade
4 tear further describes a grade 3 tear. Not only does the contrast
extend into the outer 1/3 of the anulus, but it is seen spreading concentrically
around the disc. To qualify as a grade 4 tear the concentric spread
must be greater than 30 degrees. Pathologically, this represents the
merging of a full thickness radial tear with a concentric anular tear.
The ‘evil’ grade 5 tear describes either a grade 3 or grade
4 radial tear that has completely ruptured that outer layers of the
disc and is leaking contract material out of the disc. This type of
tear, which I most likely suffered from, can cause a chemical radiculopathy
in one or both of the extremities and result in the dreaded sciatica.
There are other 'rating systems' in use which are not based on the axial CT scan, but instead upon simple radiaographic lateral and AP views. I will not go into these ofther systems but they are less harmful to the patient for the amount of radiation is much less.
 The
CT-Discogram is not a test to be taken lightly, for there is a certain
amount of risk involved, not to mention the extreme amount of radiation
exposure and the fact that it is extremely painful. In fact the
examiners will intentionally try to elicit pain from each disc they
test (provocation). The test is considered positive if the tested disc
causes you pain; especially if the pain quality is similar to your ‘everyday
type pain’ - concordant pain. Discography should only be performed
if the patient is ready to under go a surgical procedure like the IDET,
Nucleoplasty, Discectomy, or Fusion.
The
CT-Discogram is not a test to be taken lightly, for there is a certain
amount of risk involved, not to mention the extreme amount of radiation
exposure and the fact that it is extremely painful. In fact the
examiners will intentionally try to elicit pain from each disc they
test (provocation). The test is considered positive if the tested disc
causes you pain; especially if the pain quality is similar to your ‘everyday
type pain’ - concordant pain. Discography should only be performed
if the patient is ready to under go a surgical procedure like the IDET,
Nucleoplasty, Discectomy, or Fusion.
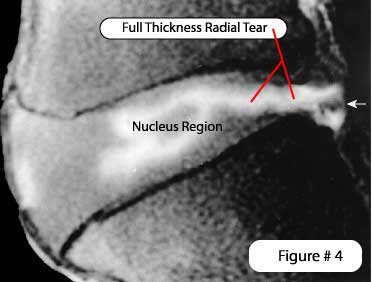
Luckily, there are other ways to see radial tears that are less invasive, although they are less accurate. MRI, especially gadolinium enhanced MRI, is also used to see these tears, and is fairly accurate. MRI discograms are even a better option for they have no radiation associated with them. Figure #4, shows a beautiful example of a full thicknes tear leading to a small disc protrusion (white arrow) as seen in this MRI Discogram.
Since the early 1970’s we have known that radial tears are directly related to disc herniations (2). Microscopic analysis of disc extrusions/protrusions recovered during surgery has shown us that extrusions/protrusions are made up of mostly nuclear material that has migrated out from the disc’s center via a full thickness radial tear. Interestingly, end-plate material, and anulus fibrosus material also is present in the make-up of disc extrusions/protrusions (33). Lumbar spinal surgery is occasionally needed to ‘decompress’ the posterior neural structures if the herniation causes cauda equina syndrome, severe pain, and/or progressive moderate to severe motor deficit.
Internal Disc Disruption: (aka: IDD)
 Another
term called internal disc disruption, or IDD, is also associated with
the radial anular disc tears described above. Figure #3
demonstrates an example of grade 4 IDD. Upon disection this would most
likely show a combination full thickness radial anular tear, comunicatting
with a large posterior concentric anular tear.
Another
term called internal disc disruption, or IDD, is also associated with
the radial anular disc tears described above. Figure #3
demonstrates an example of grade 4 IDD. Upon disection this would most
likely show a combination full thickness radial anular tear, comunicatting
with a large posterior concentric anular tear.
Although some researchers tend to use IDD and radial anular tear interchangeably, IDD is technically is more than just a radial tearing of the anulus fibrosus. It is more of a ‘Medical Diagnosis’ pertaining to discogenic back pain.
IDD was first described by Crock in 1970 (8) and again in 1986 (9). They described it as a ‘disruption of the internal architecture of the disc without signs of disc protrusions or without positive signs for nerve root compression’.
In 2003, Lee et al. reviewed the research on IDD from 1985 through 2000 (10). They summarized that of the 13 research papers on the subject, there was not much agreement on the subject. There was some agreement on what constituted a diagnosis of IDD. Here’s the factors that most researcher’s felt constituted a diagnosis of IDD: Lower back pain; a painful disc on provocative discography (concordant pain is even better); and a normal neurological examination (i.e. no loss of reflexes, no loss of muscle strength or atrophy, and no sensory loss). Other criteria for the diagnosis of IDD were not so universally agreed upon, including the presents of an HIZ sign on MRI, degeneration, desiccation, and a history of trauma. Based on their review of 15 years worth of research, Lee et al. boldly concluded that “IDD is not real, but a hypothetical disease”. This Korean group further stated “Our personal view is that IDD is a doctor-made disease, that is, [sic] an Iatrogenic Disc Disorder, which may lead to an unconventional invasive operation.”
In my humble opinion, Lee et al. are way off base with their conclusions and have absolutely no supportive evidence to make the statement that IDD is a doctor-made disease. This is pretty irresponsible medical report writing; although, everyone is entitled to their own opinion, even if it is not supported by medical research.
They are really ‘throwing out the baby with the bath-water’. Just because there is disagreement between researchers, does not mean that tears within the disc is a “doctor-made” disease and “is not real”. Read my whole page on IDD (here).
Rim Lesions | Concentric Tears | HIZ Sign | Anular Tear Home
References:
2) Schmorl G, Junghans H, “The human spine in health & disease”. New York: Grune & Stratton, 1971
3) Osti OL, Vernon-Roberts B, et al. “Annular Tears & Disc Degeneration” J Bone Joint Surg [Br] 1992; 74-B:678-82
5) Osti OL, et al “Volvo Award- Anulus Tears & Intervertebral Disc Degeneration – Spine 1990; 15(8):762-766
7) Aprill C, Bogduk N, “High Intensity Zone” - The Brit Jour Radio 1992; 65, 361-369
8) Crock
HV, “A reappraisal of intervertebral disc lesions” –
Med jour
9) Crock HV, “Internal Disc Disruption” – Spine 1986; 11:650-653
10) Lee KS et al. “Diagnostic criteria for the clinical syndrome of IDD” - Brit Jour Neurosurgery 2003; 17(1) 19-23
14) Sachs BL, et al. “Dallas Discogram Description a New Classification of CT/Discography” – Spine 1987; 12(3):287-294
15) Schellhas KP, et al. “Lumbar Disc High-intensity Zone – MRI & Discography” – Spine 1996; 21:79-86
21) Boos N, et al. “Volvo Award in Clinical Science: The Diagnostic Accuracy of MRI” – Spine 1995; 20(24):2613-2625
33) Moore RJ, “The Origin & Fate of Herniated Lumbar IVD Tissue.” Spine – 1996;21:2149-2155
© Copyright 2002 – 2015 by Dr. Douglas M. Gillard DC - All rights reserved