[Scout Image | Axial Anatomy | Sagittal Anatomy | Herniation Zones | CT Myelogram | Disc Herniation | Quiz | MRI False-Positive Rates ]
WARNING: Before you folks dive into this section of the site, it's extremely important to understand that MRI findings are only a SMALL piece of the "puzzle of pain" and are completely useless without physical examination findings, history, and years of experience in putting this stuff together. So NEVER try and second guess your physician with the information you may learn here. And remember: MRI has at least a 30% false positive rate (70% if your job is arduous), when it comes to disc protrusions. So just because you have one, don't mean that's the cause of your pain. Also note that this page does not demonstrate any pathology (cancer, fractures, swelling ect.) which is far beyond my scope of expertise. We are only looking at mechanical phenomenon, so the report generated by the radiologist is always important, for their experts at looking for pathology – although not so good sometimes at looking for mechanical problems such as this protrusions, annular tears, degenerative spondylolisthesis etc. |
Basic Anatomy:
I have already covered the axial disc anatomy ad nauseam on my
"Disc Anatomy Page."
So, please go there first if you are not comfortable with disc anatomy.
How To Tell What Disc You're Looking At: The Scout Image and More.
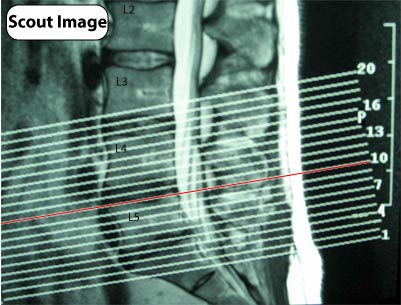 |
Without the Scout Image, it is going to be impossible for the layperson, as well as most general physicians, to discern which disc is which when viewing the all-important axial images (overhead view of the disc). It's like a roadmap that tells you which slice or current from the sagittal view (from the side) matches up with that same view in the axial plane. For example, the #10 slice in the Scout image to the left would match up with the #10 axial view, which in this case happens to run right through the bottom of the L 4/5 disc. Professional viewing software, however, like the PACs system I have at work, can display side-by-side images of the sagittal and axial views and has guidelines that move when you scroll your mouse to show you exactly where you are. |
 |
Professional viewing software, however, like the PACs system I have at work, can display side-by-side images of the sagittal and axial views and has guidelines that move when you scroll your mouse to show you exactly where you are. For example, the image to the left is a screenshot of my MRI which I have pulled up on my desktop. As I work on the axial view (far left) and scroll up and down the series with my mouse, a yellow line moves in tandem with my mouse scrolling so I always know exactly where I am. The opposite happens when I work on the sagittal images. |
 |
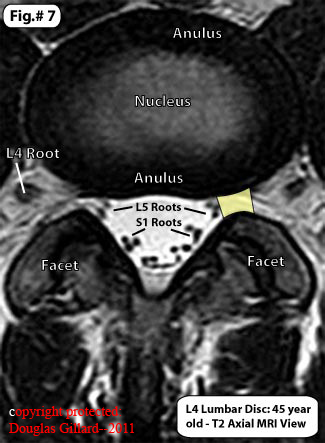
Here we have a T1-weighted axial (a view from underneath [note the left and right sides are reversed from normal]) MRI image of the L5 disc. I have put a clean copy (without writing) on the left (figure 1A) so you can practice seeing this stuff. The disc is a football-shaped structure outlined in yellow. The slingshot-like structure outlined in orange is called the posterior arch. The visible posterior arch is made up of the spinous process (those little bumps you can feel on in the center of your back), the lamina (LAM), and the facet joint (white). The facet joint itself is made up of two parts: the superior articular process of the sacrum (SAP) and the inferior articular process of L5 (IAP). The pars interarticularis (not labeled) is the region of bone between the LAM and IAP. Inside the arms of the slingshot, is called the spinal canal and contains neural tissue that looks kind of like Mickey Mouse's head. The actual head is the black circle encircled in red (TS), which represents the thecal sac (the place where all your nerve roots hang down in the structure called the cauda equina; the thecal sac is filled with cerebrospinal fluid and is the place where myelogram dye is injected and the two ears (green) represent the traversing S1 nerve roots which dive down into the sacrum and exit through the sacral foramen. The exiting L5 nerve roots' dorsal root ganglia is visible in marked in purple (DRG). You cannot see the actual exiting nerve roots – only the dorsum ganglia -- but I have drawn them in in purple (these would be seen in a series of different cuts extended upward) These exiting nerve roots leave the spine through a structure called the neural foramina (a.k.a. intervertebral foramen or IVF). The lateral recess (not labeled) is the area where the traversing nerve roots are (green circles) and is the most common site of disk herniation. The T1- weighted images do not show tissue that is filled with water. Therefore, you cannot see the nerve roots within the thecal sac, cerebral spinal fluid within the thecal sac, or even the nucleus pulposus of the disc. |
Okay, lets move on to some other stuff. Remember, if you need a over-view of the anatomy, please visit my 'Disc Anatomy Page'.
The Sagittal Image Anatomy: View from the Side.
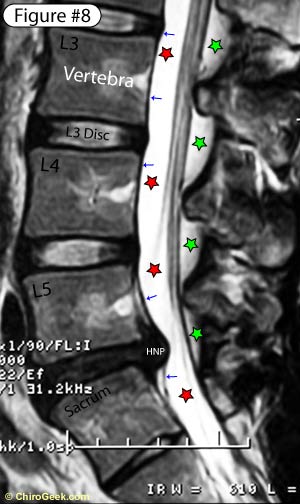 |
Figure #8 is a T2 weight MRI view of the lumbar spine from the side, or a Sagittal Image. First the basic structures: The discs, which are stationed between the vertebrae, should be a white color (hydration). Note the 'blackness' (desiccation) of the L5 disc (disc between L5 and sacrum); this represents moderate degenerative disc disease. The PLL (tiny blue arrows) appears as a black vertically orientated line running down the posterior surface of the vertebral bodies and disc. Note that, amazingly, despite this patients 9mm disc herniation (white HNP), the PLL is still 'containing' the protruding nuclear material and has not appeared to have ruptured, although it is certain uplifted from the bone, as nuclear material is seen above level of the disc space. This would technically be called a large contained disc extrusion. The thecal sac (red stars) is the 'super white' structure that fills the central spinal canal just behind the posterior vertebral bodies. This sac house the free-floating spinal nerve roots (cauda equina) and is made up of both motor and sensory nerve fiber. The ligamentum Flavum (green star) courses between each of the vertebrae and adds stability to the spine. This structure can hypertrophy or thicken in some patients and help to cause the dreaded central canal stenosis, which is the nemesis of the elderly. Look for those Nerve Roots on the Sagittal Image too: |
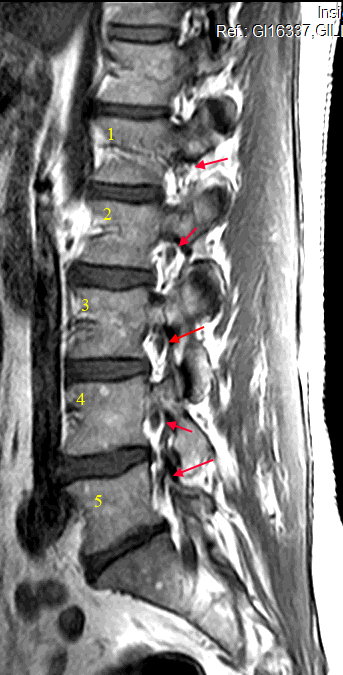 |
This is a sagittal T2 waited MRI, which is a far lateral cut (way off to the edge). This demonstrates the very important neuroforamen and the exiting nerve roots (red arrows) within them. This is a very important slice and both sides should be carefully inspected to make sure no disk herniations have occurred here. Usually disk herniations do not go into this area (the neural foramen); however, when they do, not only can they cause severe sciatica, they can also be quite difficult to reach during discectomy. |
Zones of the Anterior Epidural Space: Herniation Zones.
Now, let's use some CT axial images (my own) to learn the different regions of the anterior epidural space; the regions where disc herniation occur in. If you have ever read your MRI report, some of these terms may sound familiar, for these are regions (zones) are often used by radiologists to describe the exact location of your disc herniation.
BLUE: This is the 'Central Region' and is located directly behind the disc and encompasses the anterior aspect of the thecal sac. Since the PLL (posterior longitudinal ligament) is at its thickest in this region, the disc usually herniates slightly to the left or right of this central zone. (As a side note, I would add that if you do have a 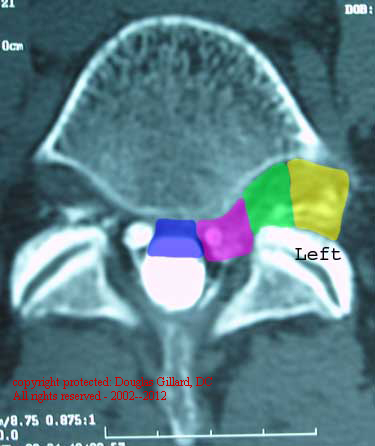 centrally located disc herniation, the chances of a successful discectomy are reduced.)
centrally located disc herniation, the chances of a successful discectomy are reduced.)
PINK: This is the 'Paracentral Region' or 'Lateral Recess' and is located just outside of the Central Region. Because the PLL is not as thick in this region, disc herniations are frequently found here; in fact, this is the number one region for disc herniations to occur in. The Traversing Nerve Roots, which are the neural structures found in this zone, are frequently contacted, deviated and compressed in this zone. (Remember, an L5 disc herniation that occur into the lateral recess with compress the traversing S1 nerve root, not the exiting L5 nerve root that lives within the IVF.)
GREEN: This is the 'Intraforaminal Zone', also known as the 'Subarticular Zone', and is located within the intervertebral foramen (IVF). It is fairly rare for a disc to herniate into this region or beyond; in fact, only 5% to 10% of all disc herniation occur here or farther out. (241-244) When herniations do occur in this zone, they are often very troublesome for the patient. This is because a super-delicate neural structure called the 'Dorsal Root Ganglion' (DRG) lives in this zone. Any compression of the DRG can result in severe pain, sciatica (aka: radiculopathy) and nerve cell body (neuron) damage.
YELLOW: This is the 'extraforaminal zone' and, as the name implies, is just outside (lateral to) of the IVF. Again, it is very rare for a disc to herniate into this region, but when it does happen, it is often very troublesome for the patient and surgeon. A herniation in this zone may also irritate the 'Sympathetic Nervous System' and cause RSD like symptoms in the lower limb.
Axial CT Myelogram: Anatomy and Herniation.
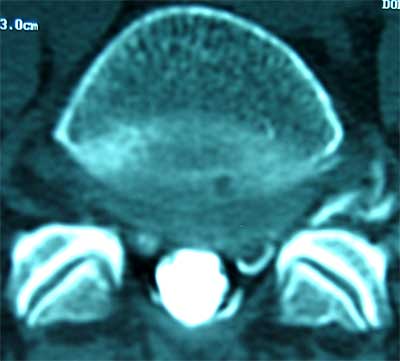
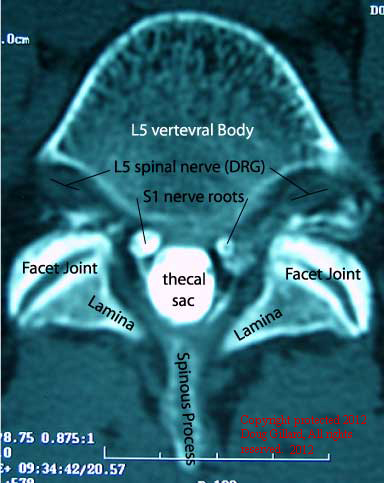 Let us now look at some CT Myelogram images (mine). The first image (left) is from a 'slice' (remember, CT and MRI images are all thin cuts through the spine in different planes) just above the L5 disc, through the inferior region of the vertebral body. Since the 'slice' is above the level of the disc, you will only see the posterior neural structures and not the disc itself.
Let us now look at some CT Myelogram images (mine). The first image (left) is from a 'slice' (remember, CT and MRI images are all thin cuts through the spine in different planes) just above the L5 disc, through the inferior region of the vertebral body. Since the 'slice' is above the level of the disc, you will only see the posterior neural structures and not the disc itself.
Note the bright white 'ring apophysis' (not labeled) that out-lines the vertebral body - more so anteriorly (top of the picture).
Note that the cauda equina (thecal sac) is completely filled with 'white' contrast material (injected during my myelogram) that makes the thecal sac (dura and arachnoid mater that surrounds the cauda equina) and the 'Dural Sleeves' (which contain the spinal nerve roots) bright white. Since the contrast only fills the root sleeves up to the DRG, the DRG of L5 is not well visualized. I've placed a black line in the center of each DRG (dorsal root ganglion).
Also note the facet joints (oblique black slits - labeled) which are sandwiched between the superior articular process of the sacrum and the inferior articular process of L5.
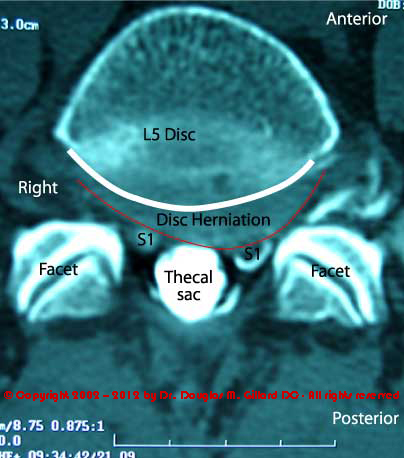 The next CT slice (right) is a little be lower than the slice above and demonstrates the posterior of the disc quite nicely. Now you can plainly see the posterior disc has both bulged and herniated into the left traversing S1 nerve root, hence blotting it out (not white in color like the right S1 is).
The next CT slice (right) is a little be lower than the slice above and demonstrates the posterior of the disc quite nicely. Now you can plainly see the posterior disc has both bulged and herniated into the left traversing S1 nerve root, hence blotting it out (not white in color like the right S1 is).
I've high-lighted the posterior ring apophysis (white thick 'smile' line) to demonstrated how a diseased disc can 'bulge' outward. Anytime disc tissue is seen outside of the posterior vertebral body (ring apophysis), the disc is considered to be 'bulging'. Bulging discs are usually no greater than 2 or 3 millimeters (mm) and are 'concentric' or 'non-focal' in shape.
My disc bulge has an out pouching or eccentric component to its shape, as noted by the portion that has moved into the left 'Lateral Recess'. This out-pouching's is the herniation component to my disc lesion, and it has made my left S1 root disappear because its failed to properly fill with contrast - probably due to compression of that root at this level. (Note the white Nike swoosh just under the "S1" on the left, affected root. This is contrast material that "accidentally" leaked into the epidural space following my myelogram. This wasn't suppose to happen be created a semi-epidurogram effect.)
 Here is that same image - the L5 disc level - without all the markings. Try and practice looking at the disc yourself without the aid of my boundary markers. Can you see the herniation? I bet you can now! This is considered a broad based herniation for its base it bigger than its anterior to posterior projection.
Here is that same image - the L5 disc level - without all the markings. Try and practice looking at the disc yourself without the aid of my boundary markers. Can you see the herniation? I bet you can now! This is considered a broad based herniation for its base it bigger than its anterior to posterior projection.
One thing to keep in mind: CT myelogram's are designed to look for 'filling-defects', and are not really the best imaging system for evaluating the human disc. The MRI is much better at visualizing the disc.
On a CT myelogram (left), if the disc herniation is large enough it will make the nerve roots turn black, or disappear (like it does to my left S1 root - only its confusing for you still see that tilted 'C' of white - which is only the outline of the black, contract-free, left S1 root). This is because the compression upon the nerve root will NOT allow the contract material to 'fill' into the nerve, hence, no bright white nerve root. That spells TROUBLE!
9MM DISC HERNIATION: A Real Case.
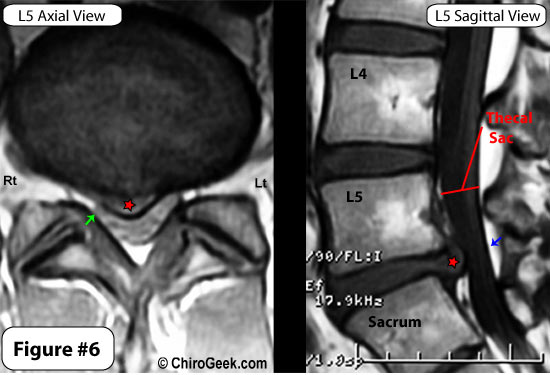
Figure #6. demonstrates a large 9mm disc extrusion (red star) as visualized on both the T1 Axial (over-head) and Sagittal (side) views.
Note that this extrusion has completely blotted out (can't see) the right traversing S1 nerve roots (left side of image) and has pinched it against the lamina (tiny green arrow). Note the thecal sac is moderately to severely compressed by this large herniation, as noted on both the axial and sagittal images (between blue arrow and red star).
This young man (24 years) has avoid surgery and is doing fairly well, although his days of heavy work are probably over for good.Note the central canal of this young man is much smaller that that of the young man in figure 10 and 11. That just pure genetic folks; bigger central canals are much more forgiving for disc herniation, that smaller ones.
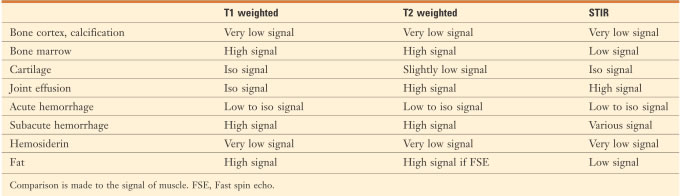
T1 vs. T2: the differences:
 Practice test: Let's see what you have learned!
Practice test: Let's see what you have learned!
1) On the below MRI axial image of the L5 disc, name the structures that are numbered.
2) Name me the location of the 'disc lesion' using the correct zone.
3) Which nerve root is being displaced by this disc lesion?
4) bonus: What type of MRI image are we looking at??
hint: T1, T2, or Proton density??
5) What two structures are being contacted by this disc lesion?
GOOD LUCK! Make sure you look at the answers via the link below. I've got the case history to go along with the quiz MRI, including his lateral view, and the official MRI report.
Get the Quiz Answers 'Here'.
References:
241) Epstein NC, et al. "Far lateral lumbar disc herniations and associated structural abnormalities: an evaluation in 60 patients of the comparative value of CT, MRI, and myelo-CT in diagnosis and management. Spine 1990; 15:534-49
242) Abdullah AF, et al. "Surgical management of extreme lateral lumbar disc herniations: review of 138 cases." Neurosurgery 1988;22:648-53
243) Kunogi J, Hasue M, "Diagnosis and operative treatment of intraforaminal and extraforaminal nerve root compression." Spine 1991;16:1312-20
244) Lejeune JP, et al. "Foraminal lumbar disc herniation: experience with 83 patients." Spine 1994;10:1905-8
Home | Top | Test Answers & Case History of Javier
© Copyright 2002 – 2012 by Dr. Douglas M. Gillard DC - All rights reserved