
annular tear: the rim lesion
| The History | a Real Rim Lesion | The Sheep Studies |
Rim Lesions in General:
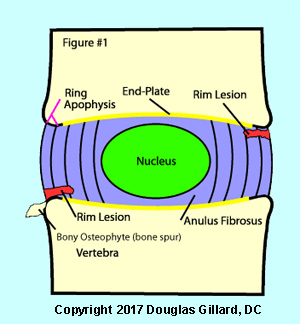 Rim Lesions (figure #1), which are also known as peripheral or transverse tears, are small annular tear which begin at the upper or lower periphery of the disc. Specifically, they occur as tears through Sharpey's fibers at their point of insertion into the bony ring apophysis.
Rim Lesions (figure #1), which are also known as peripheral or transverse tears, are small annular tear which begin at the upper or lower periphery of the disc. Specifically, they occur as tears through Sharpey's fibers at their point of insertion into the bony ring apophysis.
These tears are not thought to be related to the natural aging/degeneration process of disc, but instead are associated with some sort of trauma. There often associated with a special type of osteophyte (bone spur) called a "traction spur." Which occurs a few millimeters above the corner of the vertebral body.
It is believed they are fairly short-lived and soon progress in word until they connect with the nucleus pulposus, thereby forming a full thickness annular tear.
Rim lesions have been associated with the onset of pathological disc degeneration in several studies, as well as degeneration of the vertebral endplate and facet joints. [5, 27, 24, 30]
Especially noteworthy was the 1990, Volvo Award-winning study of Robert Moore et al (5) that demonstrated the outcome of experimentally inducing (via pin-prick or scalpel) a thin, shallow(5mm) incision into the outer annulus of an animal disc. That is, that shallow annular tear always worsened into a full thickness annular tear; the disc and vertebral end-plate would undergo rapid degeneration/desiccation; and degeneration of the posterior facet joints of that level would occur bilaterally.
 Fig. #2: Here we have a beautiful example of a rim lesion (black arrow) at the L3 disc in a real dissected human lumbar spine. on the other side of the disc, you can see a full thickness (radial) annular tear which is not quite made it through the periphery. It meets with a concentric annular tear, so this would be called a grade 5 annular tear.
Fig. #2: Here we have a beautiful example of a rim lesion (black arrow) at the L3 disc in a real dissected human lumbar spine. on the other side of the disc, you can see a full thickness (radial) annular tear which is not quite made it through the periphery. It meets with a concentric annular tear, so this would be called a grade 5 annular tear.
Note that the rim lesion has started from the very top corner of the periphery of the disc. This is what makes it a rim lesion. Furthermore, note that the rim lesion does not extend all the way into the nucleus pulposus, like the full thickness radial annular tear does on the other side of the disc.
The $64,000 question is whether or not either of these tears caused the decedent chronic low back pain. Research indicates that not all annular tear resulting chronic low back pain and we are not completely sure why some people react so poorly to their presence, while other people are not bothered by them at all.
The History of Rim Lesions:
Rim lesions were first described by Schmorl & Junghans in 1971, where they noted the common appearance of transverse peripheral tears in cadaver discs that only occurred in the periphery of the disc and were associated with small osteophytes (bone spur) formation (2). In 1984, Hilton & Ball studied 117 lumbar cadaver spines. They noted that rim lesions attempted to repair themselves by forming fibrovascular and fibrocartilaginous tissue within the tears. Amazingly they also discovered that ‘age’ did not play much of a roll in the appearance of rim lesions. In their study there were just as many rim lesions in subjects under 20 years or age, as there were over 20 years of age. This strongly indicates that rim lesions are not related to the natural aging process but most likely the result of trauma to the disc. They finally boldly stated that rim lesions were most likely a cause of back pain (23).
Enter the Sheep Studies of the 1990s:
Rim lesions have been extensively studied using sheep as a model. The sheep disc is amazingly similar to that of the human. In a nut shell, we have learned that when a rim lesion is surgically induced in a living sheep, that lesion always devastates the disc, in a fairly rapid manor. Here’s what we know so far: First, we we have learned that a small induced rim lesion (4-5mm) always worsens and completely ruptures into the center of the disc. This in turn allows nuclear material to protrude outward through the tear and into the outer regions of the disc; only to be stopped from completely leaving the disc by a 'plug' of vascularized granulation tissue. Secondly we have learned that the outer 1/3 of the rim lesion will rapidly heal with a vascularized granulation tissue. Again, it is this ‘granulation plug’ that stops the disc from completely herniating, as it holds back the nuclear material. Unfortunately, because of the avascular nature of the inner anulus, the healing process does not occur in the middle or inner anulus and has only been seen in the outer 1/3 of the disc. Thirdly, we have learned that following the induced tear, a rapid and destructive degenerative process occurs throughout the nucleus, anulus, end-plate and eventually the facet joints (5, 27, 24). The onset of this degeneration process is rapid and usually occurs by 4 months in sheep, and even faster in pigs (whose disc is the closest match of all to the human disc.) Remodeling of the subchondral bone not only occurs adjacent to the stab wound, but occurs through out the upper and lower end-plates (27). This ‘bony sclerosis’ probably severely inhibits disc nutrition by blocking the vital ‘vascular channels’ of the end-plates that pipe-line nutrients in and out of the nucleus and inner anulus, which in turn leads to rapid degeneration within the disc. This degenerative process is also associated with the development of both concentric and radial anular tears. Finally, we have learned that not only do these induced tears result in marked disc degeneration at 4 to 12 months, but they also lead to marked facet degeneration as well, although this is a much slower process 18 months. (5, 27, 28, 29)
Recently, in 2005, Kim et al. released a controlled investigation that again confirmed that needle stick injuries (with 18 and 21 gauge needles) into the outer live rabbit disc always produced rapid degenerative changes within that disc (30).
HUMAN DISC RESEARCH:
In 1992 Osti and Vernon-Roberts studied 135 human discs of cadavers. They again found rim lesions in the outer periphery of the anulus fibrosis that were parallel and adjacent to the ring apophysis. These lesions were “frequently" found to have vascular granulation tissue (scar tissue) extending into the middle annulus but no farther. They also noted that rim lesions “generally gave origin to circumferential anular tears” and were “often” associated with osteophytes (bone spurs) adjacent to the lesion (fig.#1). As far as location goes, the researchers noted that rim lesions favored the anterior portion of the disc except for the L5/S1 disc, which only slightly preferred the posterior region of the disc. Because of the histological characteristics of these lesions, they agreed with Hilton and Ball (23) that the origin of these lesions were most likely a result of trauma induced “mechanical stress”. Osti and Vernon-Roberts concluded their paper by suggesting that rim lesions precede nuclear fraying and tearing and “may influence and accelerate the degeneration of the intervertebral disc and play a part in producing discogenic pain (3).”
IMAGING: RIM LEASIONS ON MRI?
Unlike concentric tears, rim lesions may often be seen on the T2-weighted MRI scan. In a small cadaver study in 2003, Kakitsubata et al. demonstrated that 71% of rim lesions could be identified on T2 weighted FSE MRI and appeared as “linear regions of high signal intensity that were transversely oriented” to the end-plate. Only 21% of concentric tears and 67% of radial tears were noted on MRI (12).
Be careful! Don't confuse a high-intensity zone with a rim lesion! High-intensity zones will not start from the upper corners of the outer disc. They start in the middle of the disc's periphery.
CONCLUSION:
It is generally agreed upon that rim lesions have tremendous clinical importance for not only may they cause acute low back pain, but they also probably 'doom' the disc into the future development of the more deadly full thickness radial anular tear, which in some may lead to a devastating disc extrusion and chronic pain.
REFERENCES:
2) Schmorl G, Junghans H, “The human spine in health & disease”. New York: Grune & Stratton, 1971
3) Osti OL, Vernon-Roberts B, et al. “Annular Tears & Disc Degeneration” J Bone Joint Surg [Br] 1992; 74-B:678-82
5) Osti OL, et al. Volvo Award - "Anulus Tears & Intervertebral Disc Degeneration: an Animal Model" - Spine 1990; 15(8):762-766
12) Kakitsubata Y, et al. “MR Discography in Cadavers” – Clin Orthopaedics & Relat Research 2003; 407:228-240
23) Hilton RC, Ball J, “Vertebral Rim Lesions in the Dorsolumbar spine.” – Ann Rheum Dis 1984; 43:302-307
24) Moore RJ, Osti OL, Vernon-Roberts B, “Osteoarthrosis of the Facet Joints Resulting From Anular Rim Lesions” – Spine 1999; 24(6):519-524
27) Moore RJ, et al. “Remodeling of Vertebral Bone after Outer Anular Injury in Sheep.” – Spine 1996;21(8):936-940
28) Key JA, Ford LT “Experimental intervertebral disc lesions” – J Bone Joint Surg 30A:621, 1948
29) Moore RJ et al “Changes in Endplate Vascularity After an Outer Anulus Tear in the Sheep” – Spine 1992; 17(8):874-877
30) Kim KS, Yoon ST, Li J, Park JS, Hutton WC. 'Disc degeneration in the rabbit: a biochemical and radiological comparison between four disc injury model s. Spine. 2005 Jan 1;30(1):33-7.
Radial Tears | Concentric Tears | Anular Tear Home | Anular Tears Home |
© Copyright 2002 – 2005 by Dr. Douglas M. Gillard DC - All rights reserved